The IOPC also investigated each of the incidents where families suggested that police contact occurred as a result of the police listening to their telephone conversations. Investigators were able to provide family members with a plausible alternative explanation for what had occurred. These explanations were welcomed by the families, even where it could not be confirmed that this was what had happened. The IOPC identified that in some cases the manner of the police when they then contacted the families was not appropriate. In particular, in one incident where WMP officers were sent to retrieve a document that should not have been in the public domain, the evidence indicates the officers behaved in an unnecessarily intimidating way towards the family. This complaint was upheld.
The allegations of individuals being followed were in many cases too vague in terms of dates and locations to enable further investigation. However, the IOPC did look in detail into one specific allegation, where a family member was conspicuously followed by police officers for almost a week—and on at least one occasion, spoke to the officers directly. This complaint was upheld.
To investigate the burglaries, the IOPC instructed Merseyside Police to retrieve all material relating to them, from initial incident logs through to subsequent investigations, and to provide names and ranks of all officers who attended. The initial response was disappointingly slow, and the IOPC had to escalate the issue to senior officers, including the Head of Professional Standards at Merseyside Police, before receiving the material. Having looked into the matter, the Head of Professional Standards apologised to the IOPC for the poor initial response from the force and ensured more comprehensive information was provided.
This information indicated poor practice in the crime recording process, with key information relating to the crimes being recorded either inadequately or inaccurately.
Two separate burglaries—the first burglary at the Hillsborough Centre and the first burglary at the HJC shop—were recorded as one incident.
No information at all—not even a crime reference number—was found in relation to either of the break-ins at the home of the individual involved in the campaign and support group.
Despite this, the information that was available did not support the allegation that the police were in any way involved in the burglaries. Some of the recollections that only material related to the disaster was stolen proved incorrect and in one case, witness accounts described those involved in the incident as youths, indicating they could not have been police officers. This does not, however, prove the campaigner or the campaign and support groups were not under police surveillance.
The IOPC sought to examine potential explanations for the noises that people heard on their telephone lines, other than that they were a result of police surveillance. Investigators contacted three telephone engineers who had experience of supporting official surveillance during the 1990s and 2000s. They all indicated that if there had been authorised surveillance of telephone lines, the users would not have heard anything. This was because of the way such surveillance was conducted. They also suggested that in this period, crossed lines—that is, hearing a different conversation—sometimes occurred as a result of either a fault or water ingress on the line.
The IOPC also appointed an expert witness on surveillance, who had been part of the surveillance team at the Metropolitan Police Flying Squad. He was asked to comment on various matters, including the noises that complainants had heard on their telephone lines. He said that, as far as he was aware, authorised interception of communications took place in a sterile environment where “it would be impossible to hear intruding voices.” He also observed that if voices could be overheard during an interception operation, it “would completely jeopardise and compromise the process.” He could not offer an explanation for the clicking noises heard.
Together, these responses indicated that the noises were unlikely to be a result of official police surveillance.
To investigate the allegations, the IOPC began by taking statements from family members and others about what they had experienced and why they thought this could be a result of police surveillance. The issues most commonly cited related to problems with telephone lines.
Twenty-one of the complainants who wrote to the IOPC reported hearing noises, such as clicks on the line, when they made or received telephone calls at home. Some also said they often experienced a delay at the start of a call. All suspected these noises and interruptions were the result of telephone interception carried out by, or at the instruction of, the police.
In some cases, the noises continued even after the individuals had moved home or changed telephone provider.
One complainant said that, in one property he lived in, he only heard these noises when speaking to another individual who wrote to the IOPC.
One woman only heard noises when she called her mother, who was a prominent member of one of the campaign and support groups related to the disaster. Her concern was not about her own telephone line being intercepted, but rather her mother’s.
Four people referred to a specific crossed-line incident, which meant two individuals overheard, during a call between them, the separate telephone conversation of a third complainant. All already knew each other as a consequence of the disaster.
Eight further individuals referred to hearing other voices on the line. Three of these (including two who referred to calls made from a public phone box near SYP HQ) specifically mentioned hearing sounds that were like police radio or other police conversations.
In some cases, family members had some form of contact with the police, which they believed occurred as a result of the police hearing something they had said in a phone conversation.
Understandably, those reporting the issues were often not able to state which police force, or forces, could have been involved. There was also no information on surveillance in the archives, or in the material disclosed to the HIP.
Five complaints referred to burglaries in Merseyside, as well as the interception of communications. Two of these incidents were at the Hillsborough Centre—set up to provide support to families and supporters who had been at the match—and two at the Hillsborough Justice Campaign (HJC) shop. A further two incidents, covered by the same complaint, took place at the home of a member of the HJC. Because in each case material that was stolen or damaged involved information relating to the disaster and the work of campaign and/or support groups, the complainants raised the possibility that the police were involved in the burglaries. This was on the basis that they felt only the police would have found the information of value.
The IOPC secured the support of the Home Secretary to ask all police forces to search for any records of surveillance related to family members of those who died, or to members of campaign and support groups related to the disaster, and to provide those records to the IOPC. No records were found. Again with the support of the Home Secretary, the IOPC then asked forces for all information they held related to the disaster, as a means of checking that nothing had been overlooked. Still no relevant information was provided.
While this could indicate that there had been no authorised police surveillance of the individuals, it could also mean that the records had been (correctly) destroyed after they had been held for the permitted period.
In relation to telephone surveillance, the legal framework meant that, at the time the IOPC made this request, records should have existed of every lawful police interception of telephone communications since 2000, and of every time a police force applied to the Home Secretary to intercept telephone communications. However, the longstanding government policy is that the Home Secretary will neither confirm nor deny whether any individual is the subject of telephone interception.
Instead, families were directed to contact the Investigatory Powers Tribunal (IPT), an independent public body which oversees complaints about the use of intrusive powers such as phone-tapping by intelligence services, law enforcement agencies and public authorities. It has the authority to view the details held by the Home Office of all authorisations granted to intercept telephone communications and to award damages to complainants.
Police surveillance powers in the UK are subject to a range of regulations. These regulations evolved over the period covered by the allegations, reflecting changes in lifestyle and technology. They have changed further since the start of the IOPC investigation.
However, there are some key principles that have remained at the core of the regulatory environment throughout. These include that all police surveillance has to be authorised, typically by senior officers, and that intercepting telephone calls is a particularly intrusive form of surveillance, which can only be authorised in strict circumstances by the Home Secretary.
The IOPC’s terms of reference included investigating:
Complaints and recordable conduct matters about police surveillance and covert activity linked to the Hillsborough disaster involving family members of those who died, survivors and other complainants linked to the disaster.
What was found?
• By 2014, no police force had any records of surveillance of the families of those who died in the disaster. However, one explanation for this could be that records had been (correctly) destroyed after they had been held for the maximum permitted period.
• In line with longstanding policy, the Home Secretary would not confirm or deny whether anyone had been subject to telephone interception (‘phone tapping’) by the police. However, families were directed to the public body that could answer this question.
• In the view of various expert witnesses, the descriptions of intrusive noises during telephone conversations did not indicate that families were subject to lawful surveillance by the police. They all indicated that the subjects of police telephone interception would not hear noises on the line as a result.
• The IOPC was able to provide some families with detailed explanations of incidents involving police intrusion on their everyday lives. Though this explained why the police were involved, it did not justify the manner of police interaction, particularly in one case where officers from WMP were intimidating.
• In one case, an individual appears to have been under overt surveillance by the police for over a week, without good reason. It has not been possible to investigate all instances where people complained they were followed by the police.
• Some of the incidents cited as indicating police surveillance were not properly recorded or handled by Merseyside Police at the time. This appears to have been the result of errors or poor practice, rather than an attempt to conceal police involvement in the incidents.
Significant new evidence
Almost of all the evidence around alleged surveillance was new, as these issues had not previously been looked at. The IOPC took statements from a large number of witnesses describing their experiences and why they suspected these to have been a result of police surveillance. In addition, the IOPC contacted expert witnesses in telephone interception, from both the policing perspective and the telecommunications industry. Further, the IOPC used its powers to obtain documents from Merseyside Police, after its initial response to requests for information had been insufficient.
Over the years since the Hillsborough disaster, there have been repeated allegations that family members of those who died, and members of campaign and support groups related to the disaster, were placed under surveillance by the police. The alleged surveillance ranged from telephone interception (that is, that their phone lines were ‘tapped’ so that others could hear their conversations), to individuals reporting being followed. There were also suggestions that:
there may have been some form of police involvement in break-ins at homes or Hillsborough-related locations, whether to intimidate campaigners or obtain material related to the disaster and subsequent campaigns
the police intruded in different ways on the everyday life of bereaved families
After the IOPC investigation into the aftermath of the disaster was first announced, the issue of alleged surveillance was raised in Parliament, with MPs representing constituencies where many families lived asking for an investigation into the matter. The then Home Secretary, Theresa May, agreed that it should be considered by the IOPC, and it was added to the terms of reference.
The IOPC received 27 complaints relating to alleged police surveillance and/or covert activity, from 25 complainants with connections to the Hillsborough disaster. All 25 alleged that some of their or their families’ telephone conversations had been intercepted by, or at the instruction of, the police.
In 16 of the complaints, there was also a further allegation of surveillance or covert activity, such as an individual being followed by police officers, or of police intrusion in their family life.
The complaints covered a long timeframe. The earliest referred to incidents around the time of the Taylor Inquiry (1989–90) and the most recent involved noises heard on telephone lines during 2015. They also referred to the alleged actions of officers from a number of forces, including Merseyside Police, SYP, WMP and the Metropolitan Police. In several cases, the complainant was not able to identify any particular officer or force involved.
While SYP’s actions appear to have been in line with what might be expected, the IOPC has identified a series of concerns about the thoroughness of the WMP investigation and the records WMP made relating to it.
This investigation was led by Detective Chief Inspector Kevin Tope (DCI Tope), who began by taking signed statements from the four key witnesses, followed by further statements from the technical consultant and police officer who worked in the SWFC control room.
On 13 May 1989, DCI Tope submitted a report in which he wrote that, despite making “full enquiries” at the ground including a “thorough search”, the tapes had not been found. However, there is no documentary evidence of what searches took place.
Given there were no signs of forced entry, this would tend to suggest that the room had either been left unlocked by the technical consultant or the head of security, or that it had been unlocked by someone else. WMP did not establish who had access to keys. There are indications in the existing accounts that there was at least one more set of keys, kept in Mr Mackrell’s office, but the IOPC has not been able to confirm this, nor who would have had access to them. There is nothing to suggest that WMP attempted to interview Mr Mackrell about this or any other aspect of the tapes’ disappearance.
No WMP officer contacted DS Oughton to ask him for further details of his initial steps.
Finally, the notes from DCI Tope on the action mentioned that “Supporters, relatives, press etc had virtually unrestricted access to stadium on 15.4.89 due to disaster.” This comment appears to imply that any of those—or indeed, any other member of the public—could have removed the tapes. However, it overlooks some key points:
according to several witnesses the room was locked
there is no obvious reason for any of these individuals to have known that the facility even existed
SYP officers and SWFC staff also had unrestricted access to the stadium
DCI Tope died in 1992. The IOPC has not found evidence of any occasion where he was asked about the investigation he conducted into the missing tapes.
While there are reasons to question the rigour of the investigation he conducted, there was insufficient evidence available 30 years on to ascertain exactly what steps he did take. This meant that the IOPC could not answer whether his investigation reached the standards that a competent detective could reasonably be expected to have achieved.
There is also some indication of disquiet or frustration among SYP officers about the way WMP investigated the disappearance of the tapes.
On 10 May 1989, D Ch Supt Addis sent ACC Anderson a report around the disappearance of the tapes. In it, he noted that the SYP officer who worked in the SWFC control room had been interviewed three times by WMP, “who, it appears, seems somewhat dissatisfied with our officers explanations.” In a statement to Operation Resolve, he reiterated his concerns about this and commented that it appeared the SYP officer “was their only suspect.”
In relation to the bigger picture, the IOPC also found no evidence to suggest SYP was involved in any cover-up, or indeed in the disappearance of the tapes in any way.
On Monday 17 April, DS Oughton of SYP was instructed to obtain all video footage taken by SWFC on the day of the disaster, as part of SYP’s work to preserve evidence. By this stage, SYP had already secured its own video tapes from the PCB for review. These were passed to WMP once it took over the investigation. This was all fully documented.
DS Oughton phoned SWFC and was told by a solicitor working for the club that all the tapes were in a locked safe at the ground, but that SWFC was not yet willing to release them. Later that same day, the solicitor phoned DS Oughton back and told him two of the tapes were missing.
On 18 April, DS Oughton visited the ground where he met the technical consultant, who showed him the recording system and described what had happened. DS Oughton made a report of this visit. He noted that the technical consultant said he had ejected the tapes, locked the room and set the alarm, then returned the following morning at 9am and found the tapes missing.
In his report, DS Oughton commented that there were no signs of forced entry to the room or to the cupboard where the video recorders were kept.
SYP did not conduct any further enquiries. Shortly after this, SYP handed over responsibility for all investigative actions related to the disaster to WMP and did not investigate the disappearance of the tapes further.
However, the evidence of this initial period indicates that SYP had acted promptly and professionally in relation to the issue. Further, the fact that SYP had already prepared its own videos for investigation—which were potentially far more damaging for SYP than SWFC’s footage—indicates it is unlikely that SYP would then seek to prevent SWFC’s tapes being made available.
Investigators re-examined the documents and evidence gathered as part of the original investigation, establishing what steps SYP had taken before it passed responsibility for the investigation to WMP. They then looked at the WMP investigation, as well as reviewing statements made to different inquiries by key witnesses such as the technical consultant. It was not possible to conduct any forensic examination at this stage. However, the IOPC did take new witness statements from some of those who had been involved in the original investigation into the disappearance of the tapes.
The available evidence did not enable the IOPC to find the tapes, or to shed any further light on who removed them.
The review of all previous materials showed a lot of agreement about the core facts among four main witnesses—the technical consultant, his recently appointed successor who was in the control room as an observer, a police officer who typically worked in the SWFC control room on match days and SWFC’s head of security.
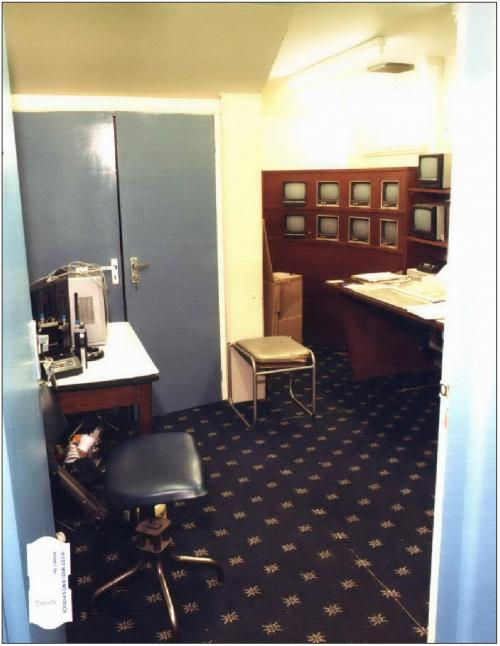
The technical consultant had revamped SWFC’s CCTV system a couple of years previously. It involved a network of cameras positioned around the ground. Each camera was connected to a dedicated monitor in the control room, which was located in the South Stand, in an area of the stadium to which the public did not normally have access.
There was a video recorder (sometimes referred to as a video cassette recorder, or VCR), linked to each of the monitors, which recorded the camera’s output on match days. These were standard video recorders, placed on shelves in a cupboard in the control room. Both the cupboard and the room itself were lockable, using separate keys. There were further keys to operate the alarm system for the room and to turn the computer and CCTV system on.
Image
Figure 18A: Screens and lockable cupboard in the SWFC control room (Source: WMP)
Image
Figure 18B: Video recorders inside the lockable cupboard (Source: WMP)
The technical consultant and police officer both recalled that the tapes had started recording as normal on 15 April, sometime between 12.30 and 1pm.
There was agreement that someone was in the room from the time the tapes started recording until 6pm.
By the time the tapes stopped recording late in the afternoon, the stadium was empty. In what he highlighted as a change from normal practice, the technical consultant ejected the tapes from the video recorders but left them resting in the carriages of the video recorders (that is, half in, half out). He has given two different explanations for this. In a statement he gave to SWFC’s solicitors, he stated he did this “so that I could later know exactly which tape related to which monitor/area.” At the Goldring Inquests, he suggested that ejecting them made sure they could not be inadvertently recorded over.
While no one in the room has stated categorically that all the tapes were there at this point, no one has indicated that any were missing.
There are some differences in accounts of what happened after 6pm, when the police officer and successor to the technical consultant both left. The technical consultant has stated he turned the alarm on and locked up but then had to return to the room to produce some printouts from a computer. The head of security has also said that he went into the room to retrieve his coat—though in a different account, suggested he picked up his coat from elsewhere. This all happened before 7.30pm.
Both had their own set of keys to the room. Neither specifically stated that they locked everything up again.
The technical consultant has consistently stated that he discovered the tapes were missing when he returned to the ground at around 9am the following morning. He has stated that the control room door was locked when he arrived, but the door to the video recorder cupboard was ajar and two of the recorders did not have tapes in them. At some points, he has stated the alarm was working when he arrived but in his most recent account, a statement to Operation Resolve, he said the alarm was not set.
After discovering the tapes were missing, the technical consultant has consistently stated that he first searched the room for the two missing tapes, then reported the loss to Mr Mackrell. In some accounts, he has said he also informed the SWFC Chairman, Herbert McGee, at the same time.
Though the technical consultant discovered the tapes were missing on the morning of Sunday 16 April 1989, SWFC did not immediately report their disappearance to SYP.
The IOPC’s terms of reference included investigating: The allegation that SYP may have been involved in the removal of video tapes from the Sheffield Wednesday Football Club (SWFC) CCTV room between 15 April 1989 and 16 April 1989, and the following specific conduct matter regarding the investigation conducted by WMP Detective Chief Inspector Kevin Tope (DCI Tope):
a) that DCI Tope failed to conduct an effective, thorough, and complete investigation into the alleged theft of two video tapes from the SWFC CCTV control room and, in doing so b) that DCI Tope failed to secure and preserve evidence, pursue relevant and obvious lines of enquiry and interview key witnesses
What was found?
• The IOPC found no evidence to support the suggestion that SYP was involved in the removal of the video tapes. In fact, the evidence indicates that SYP acted promptly and professionally when looking into the matter.
• SWFC did not alert SYP to the tapes’ disappearance immediately. When a detective first asked for them, he was told they were in a safe at the stadium.
• There was no sign of forced entry into the video room or the lockable cupboard in the room where the video recorders were. There remains some uncertainty over who had keys to the room.
• There appear to have been multiple shortcomings in WMP’s investigation into the disappearance of the tapes, or at least the records it made of the investigation. These included the fact that there was no evidence to suggest that WMP made efforts to question SWFC officials who had access to the room.
• There is some evidence that SYP officers were critical of WMP’s approach to the matter.
Significant new evidence
Beyond some witness statements, the IOPC did not obtain new evidence in this strand of its investigation. However, WMP’s investigation into the disappearance of the tapes had not previously been re-examined. IOPC investigators were able to assess in detail the actions WMP took.
Shortly after 9am on 16 April 1989, a technical consultant working in the SWFC control room at Hillsborough Stadium reported to club officials that two video tapes, which would have held CCTV footage recorded during the afternoon of the disaster, were missing. The tapes were among 16 believed to have been recorded by SWFC on the day of the disaster, in line with its standard approach of recording the footage of all matches held at the ground in case it needed to be reviewed. The consultant said he had left them in a locked room at the stadium overnight.
Despite investigative work being undertaken by both SYP and WMP, the tapes have never been found. It has been widely alleged that they were stolen, at some point between late afternoon on 15 April 1989 and 9am on 16 April. Further, because one of the tapes should have held footage showing he area around Gate B and turnstiles 9-12 at the Leppings Lane entrance, which would have been directly relevant to investigating the disaster, it has been suggested that they could have been removed by SYP.
The disappearance of the tapes became public knowledge when it was referred to in the 1996 ITV docudrama ‘Hillsborough’. The incident was then further examined as part of the Stuart-Smith Scrutiny the following year, which concluded that, while there was no dispute that the tapes had been stolen, they would not have provided any new significant evidence.
For many of those who had raised concerns about the disappearance of the tapes, there was a view that questions remained unanswered. This was demonstrated when the IOPC received a complaint about the issue after it had started its investigation. The IOPC therefore added the disappearance of the tapes to its terms of reference, specifically focusing on the allegation that SYP could have been involved in the removal of the tapes.
The final aspect of WMP’s work in relation to the Popper Inquests that the IOPC investigated was the preparation for the generic hearing. This began in earnest after the DPP’s decision in August 1990 that no charges would be brought against anyone in relation to the disaster. The generic hearing then began in November 1990.
Throughout this period, Dr Popper continued to ask WMP for advice and assistance on a range of matters, as is typically the case with coroners preparing for an inquest of any size. The evidence available to the IOPC does not indicate that WMP overstepped the mark in the work it undertook, or in providing their views where they were asked for.
Nonetheless, it was notable that in a report produced after a meeting of WMP’s Hillsborough investigation management team on 31 August 1990, there was a suggestion that Dr Popper may want to examine “the amount of drunkenness and unruliness during the build up to the crush outside the ground at about 1420 hours onwards.” This was in the context of a discussion around the evidence that should be heard at the generic hearing. In relation to this, the officers advised Dr Popper: “we would suggest that you concentrate on the period between say 1420 hours when the crowd had noticeably built up, through to Superintendent Greenwood running on to the pitch at 1505 hours plus to stop the match.”
These points appeared to suggest that, in WMP’s view, events after 3.05pm had no impact on how people died, but alcohol consumption before 2.20pm may have done.
At a meeting with WMP a few days later, Dr Popper stated his intention to hear evidence up to about 3.20pm but also that “he would hear evidence for example, on the routes, the pubs, local residents etc.”
It is not clear that this was a result of WMP’s recommendation in its report of the earlier meeting. Some documents indicate that Dr Popper was already considering hearing evidence about these topics.
One of the central questions the IOPC sought to investigate in relation to WMP was whether it displayed any bias towards fellow police officers in its work. The IOPC identified one occasion in the preparation for the generic hearing where it appears ACC Jones shared information with SYP that he did not share with other parties. This was when he gave ACC Anderson a list of SYP officers who it was proposed to call as witnesses. No evidence has been found to suggest that a similar list of staff likely to be called was shown to SWFC or any other organisation.
This was one of the handful of instances identified by the IOPC across the whole of WMP’s work where ACC Jones appeared to favour SYP in some way.
Taken as a whole, the work conducted by WMP in support of the Popper Inquests was largely in line with expected standards. WMP officers went to great lengths to track the movements of those who died on the day. When Operation Resolve conducted the same exercise 25 years later for the Goldring Inquests, using more advanced technology and additional evidence, it found that a substantial share of WMP’s work on tracking movements had been accurate.
Though WMP officers advised Dr Popper, the evidence does not suggest this was inappropriate. Further, the main allegations around the Popper Inquests have not been proven. Though there were errors in some of the summaries produced for the individual inquests, these do not appear to have been deliberate. The evidence also does not support that WMP overstepped the mark in seeking to secure further statements from two key witnesses.
At the generic hearing, the jury returned a verdict of accidental death for all of the 95 who had died by this point. The evidence does not suggest that WMP had any inappropriate influence on the process, or the outcome.