Supporters complained that some WMP officers were rude or intimidating, or that they did not seem interested in what they had to say. For example, one witness told the IOPC: “One officer sat down and the other stood up in front of me, with his hands in his pockets for the whole time he was in my house.”
In May 1989, WMP also received a complaint about the manner of its officers in Sheffield. A young man, who was a student in the city and had been at the match, responded to the witness appeal and agreed to go to a police station and provide a statement. However, when he was interviewed, he was upset by the manner of the questioning and what he felt were unfair allegations.
He detailed his experiences in a letter to his mother. These included one of the officers adopting an aggressive manner and appearing not to believe his account, to the extent of expressing doubt that he had even been at the game, because he had no injuries.
The man’s mother showed the letter to his godfather, who was a former detective chief superintendent. The godfather then wrote to WMP to complain. This was not recorded as a formal complaint, but ACC Jones instructed D Ch Supt Foster to “Initiate a follow-up to smooth troubled waters.” [Emphasis in original.] The officers who had conducted the interview were contacted and responded that they thought the young man’s evidence had been inconsistent and that he was ‘anti-police’.
On 19 June 1989, D Ch Supt Foster wrote back to the man’s godfather on behalf of WMP and told him that he had spoken with the two officers in question. He further explained that the WMP team as a whole had dealt with approximately 4,000 supporters as part of their enquiries, and that this was the only incident where someone had raised concerns. While there was in fact some evidence of other supporters expressing concerns about WMP’s approach, very few raised such concerns to WMP at the time.
The man complained to the IOPC about the WMP officers who had interviewed him. Having reviewed the evidence, the IOPC upheld his complaint that WMP had recorded his comments inaccurately and incompletely, with several material errors in the accounts they drafted. The IOPC also upheld, in relation to one of the two officers, the man’s complaint that during the interview process, he was accused of lying and was intimidated and threatened with charges of wasting police time.
Complaints about specific interactions between WMP officers and individual witnesses are inherently difficult to investigate. The interviews were not audio- or video-recorded, so the only documentary evidence from the time is the questionnaires or statements themselves. The IOPC has sought to contact the officers involved; not all have agreed to speak to investigators, as is their right, but those who have replied denied behaving inappropriately.
The IOPC has also looked at the evidence of the wider work undertaken by each pair of officers complained about. In all of the cases, there was no documentary evidence or witness evidence to suggest that these officers were repeatedly or consistently rude, intimidating or biased.
It is apparent that some interviews ended acrimoniously or abruptly, where witnesses were upset or angered by the questions, or simply by the emotional trauma of recalling the events. While clearly this is regrettable, it is also not surprising that this happened on occasion, given the number of interviews conducted by WMP and the nature of the matters under investigation.
This does not alter the fact that some supporters were sufficiently upset or shocked by WMP’s behaviour that they wished to complain.
These issues were undoubtedly of deep significance to those affected. In some cases, the manner of evidence collection added to the trauma of being present on the day; for others, it damaged trust in the integrity of the investigation into the disaster.
However, the broader picture demonstrates that these issues were experienced on an individual level rather than a systemic one. Further, the overall body of evidence does not support the allegation that WMP deliberately lost, inaccurately recorded, amended or mishandled witness accounts.
The evidence in relation to the seven complaints that WMP interviewed young witnesses (under the age of 18) in an inappropriate way was more clear-cut.
One complainant, who was 15 at the time, described being so upset that his mother intervened. Another person who was also 15 at the time recalled being stopped by police officers on his way home from school, and being asked to get in the police car, where he was interviewed; a family member spotted this and intervened. A third teenager recalled being interviewed by two WMP officers at home when his parents were out. He was asked a series of leading questions and said the officers were aggressive.
Guidance at the time stated that when the police interviewed anyone under the age of 18 as a witness, there should have been an appropriate adult present. However, this was only guidance and not a requirement; it appears this was not always followed by WMP officers working in Merseyside in the aftermath of the disaster.
By contrast, the IOPC established that the ‘house to house’ questionnaire used by WMP officers when interviewing local residents in Sheffield had advice printed on it to the effect that no questionnaire should be taken from a juvenile. No such advice was included on the questionnaire used for interviewing Liverpool supporters, or indeed on the other supporter questionnaires.
Regardless of the instructions, officers should have been sufficiently alert to recognise when witnesses were vulnerable or where a traumatised witness had become too distressed to continue the interview.
As a result, the IOPC upheld all but one of the complaints about WMP interviewing under 18s without an appropriate adult present.
It should be noted that WMP interviewed many under 18s in relation to the disaster; some in the company of a parent or other adult, some on their own. The majority of these did not lead to complaint. This may suggest that in other instances, the interviews were conducted more sympathetically.
The IOPC investigated 15 complaints about WMP focusing disproportionately on alcohol, but more than 200 respondents to the witness appeal commented on it. This indicates a widespread perception among Liverpool supporters that questioning around this topic was excessive. One supporter told the IOPC, for instance, that WMP officers “continually asked questions about alcohol things like ‘did we drink on the coach’ ‘did we see anyone else drinking’.” Another commented: “Very quickly I became concerned that the questions they started to ask me were focused on drinking before the game.”
When shown the questionnaires completed in their name, several supporters noted the discrepancy between their recollection of the interview and the written record. For example, one said: “although the questionnaire only actually has a few questions about alcohol, it is my clear recollection that they asked me many, many more questions about drinking.”
As set out at paragraphs 14.40–14.41, just four questions out of the 54 in the supporters’ questionnaire could be deemed to refer to alcohol and none of these asked supporters if they had drunk alcohol. This raises various possibilities:
WMP officers went ‘off-script’ and asked additional questions about alcohol, either as a result of instruction or their own perspectives
WMP officers made additional efforts to ensure that they asked the questions about alcohol as these were deemed more important
due to the sensitivity of the topic, supporters particularly remembered WMP asking questions about alcohol consumption more than any other topic of questioning
No WMP officer has said they asked extra questions about alcohol or in any way prioritised asking about this topic.
Beyond the questionnaires and statements, there is no written record of what WMP officers asked or what witnesses said. This lack of evidence meant that in most cases it was not possible for the IOPC to uphold complaints about WMP officers focusing disproportionately on alcohol when interviewing supporters. Nonetheless, there remains a clear gap in perceptions between supporters, many of whom (not just those who made a complaint about it) recalled repeated questioning about alcohol consumption, and WMP officers, who suggested it was just another topic they covered.
The IOPC asked WMP officers who had been based in the Liverpool office about the briefings they were given and, in particular, whether there were any ‘informal’ instructions to ask about alcohol consumption. With one uncorroborated exception, officers did not recall any such formal or informal instruction.
The IOPC’s analysis of the evidence collected by each pair of officers did show that some officers recorded more information about alcohol consumption than others. Similarly, in analysing the responses to the witness appeal, there were some pairs of officers about whom there were more concerns or dissatisfaction, related to asking questions about alcohol. However, there were no pairs of officers who stood out as being subject to substantially more concerns, or as having recorded substantially more information about alcohol consumption.
Senior WMP officers have stated to the IOPC that they believe it was appropriate to ask questions about alcohol consumption in the questionnaire. It was identified early as a necessary line of enquiry, particularly given the media coverage which had suggested the level of alcohol consumption among supporters was a factor in the disaster. Furthermore, several of these senior officers have argued that the evidence WMP gathered about this issue helped Lord Justice Taylor to reach the conclusion that it was not a factor.
The IOPC fundamentally accepts that, in a set of circumstances where alcohol consumption had been publicly and widely identified within days of the disaster as a potential causative factor, it was necessary to ask supporters about this. However, this would not have extended to asking supporters aggressively or insistently about the subject.
Further, the questions included on the questionnaire appear of limited value in addressing the issue. They offered no insight into whether any alcohol consumption that was witnessed was different from normal.
In short, even though the IOPC has not been able to uphold the specific complaints on the subject, the evidence shows WMP investigated this important topic inappropriately and ineffectively.
Complaints about inaccurate recording of responses included witnesses identifying that some information they gave to WMP, which they believed was important, had not been included in the written accounts. This missing information included, for example, comments about their experiences at the 1988 FA Cup Semi-Final at Hillsborough Stadium and criticisms of the police operation. In another case, the witness recalled saying to WMP officers that he had seen other supporters “drinking cans of Coke” but in the questionnaire they had written that he “saw a few Liverpool fans drinking from cans.” As he noted to the IOPC, this completely changed the meaning. The IOPC agreed and upheld his complaint about the inaccurate recording of his comment.
Other complainants said that WMP officers had used words in writing up their accounts that the witnesses themselves would not have used. The IOPC fully accepts that this would have occurred. A witness account, whether a CJA statement or a questionnaire, does not have to be a continuous verbatim record of what the witness said, especially where the interview was not audio-recorded, which was the case with the interviews conducted by WMP. It was, and still is, common practice for police officers to use alternative forms of words, or to omit digressions and asides, to make the account easier to follow.
Given the length of interviews, and the fact that questionnaires were designed for information gathering rather than composition of a statement, it is perhaps inevitable that WMP officers sometimes edited what was said. As a result, most complaints about WMP phrasing accounts using different words to those the witnesses used have not been upheld.
Further, it is not clear that any amendments to the wording of witness accounts negatively affected the overall quality of evidence collected from Liverpool supporters. In particular, the evidence does not suggest that interviewing officers consistently and deliberately failed to record information about specific topics.
As an example of this, across all the questionnaires and statements WMP took from supporters, IOPC investigators identified more than 3,000 comments that were in some way critical of police actions on the day. While some pairs of officers recorded more critical comments than others, every pair recorded at least one.
This suggests that while it is highly possible that some criticisms of the police were not fully recorded, this was not the result of a systematic approach to avoid recording criticisms. In almost all of the cases where complainants raised this issue, the completed questionnaire did include some criticism or negative comment about the police operation.
WMP’s operation in Liverpool was based at Smithdown Lane Police Station. This was the headquarters of Merseyside Police Traffic Division. On 30 April 1989, in the early stages of evidence gathering, there were at least 120 WMP officers based in Liverpool. Broadly, this divided into six serials, each consisting of an inspector, two sergeants and up to 20 PCs. Superintendent David Thursfield (Supt Thursfield) was the head of the Liverpool operation.
During the initial phase of about three weeks, the WMP officers were, in general, working 12-hour shifts for six and sometimes seven days a week to take accounts from as many witnesses as possible. In total, WMP recorded 3,885 questionnaires from Liverpool supporters and 151 questionnaires from coach company owners or drivers who had taken supporters to the game. The majority of these were completed before 30 May.
Once the Taylor Inquiry hearings began, the operation in Liverpool was scaled back; by 4 June 1989, there were just 33 WMP officers still in Merseyside.
There is no single document setting out how WMP should, or did, gather information from Liverpool supporters. However, the accounts of the officers involved are reasonably consistent in describing the basic process, which is summarised below.
Supporters contacted WMP by phoning the dedicated freephone number for the IIC. WMP call handlers used a short questionnaire to gather initial information, including the caller’s name, contact details and where they were on the day of the game. These were reviewed in the WMP MIR, and actions were raised for officers based in the Liverpool office to go and interview the supporters.
Officers in the Liverpool office worked in pairs to conduct face-to-face interviews, using the standard questionnaire. In most cases, the officers telephoned the supporters in advance and arranged a time to interview them. Some supporters who responded to the witness appeal indicated that WMP had turned up at their door without prior arrangement. WMP officers acknowledged in interviews with the IOPC that this had happened on occasion; however, they suggested that this was when they had not been able to contact the witness in advance.
The officers were not required to inform witnesses that they were completing a questionnaire and, in general, it appears that they did not. Officers also did not necessarily ask each question in turn; sometimes supporters gave answers to one question which meant a later one was not necessary or appropriate.
If a witness indicated that they had gone to the match with someone who had died, or they had been involved in trying to rescue or resuscitate other supporters, the WMP officers took a CJA statement. They also took statements in some other cases, where they deemed it relevant or were instructed to do so.
All questionnaires and statements were submitted to the MIR. They were read first by more senior officers so that any immediate actions could be raised. The documents were subsequently typed up and recorded on the HOLMES database.
Further interviews were conducted if necessary to confirm some details or request extra information, or to take a CJA statement. It appears that where this happened, it was not necessarily the same officers who returned; if the witness had made a complaint or was being visited again in relation to a complaint from another witness, more senior officers were often tasked to make these additional visits.
The evidence available to the IOPC suggests a similar process was used for questionnaires of Nottingham Forest supporters, though only 269 of these were completed.
Based on documentary evidence from the time and the statements of former WMP officers to the IOPC, it is apparent that WMP initially underestimated the scale and complexity of the task. Though some interviews were conducted by detectives and more experienced officers (including inspectors), the majority were conducted by comparatively junior officers. They were required to interview deeply traumatised individuals about their experiences very soon after the traumatic event. Many of these junior officers had no specialist training in interviewing vulnerable people and received only limited briefings.
In statements to the IOPC, former WMP officers noted that, unsurprisingly, some supporters did get upset or angry, particularly at certain questions. Officers told the IOPC of the approaches they had taken to minimise the distress. For example, some sought first to let the interviewee simply give their account, unprompted; the officers would note down details at relevant points on the questionnaire, then ask questions to fill in any gaps. Others chose to adhere to the questionnaire as closely as possible and then use the more open questions at the end to let supporters speak more freely and provide their own recollections.
One consequence of these difficulties was that interviews would typically last longer than had been assumed in WMP’s initial calculations. Officers recalled spending several hours in some households, particularly where more than one member of the household had been at the game.
Numerous supporters also described the long process; some indicated that they had found the WMP officers to be sympathetic. This was reflected in the responses to the witness appeal, where more than 800 witnesses answered the question whether they believed the account they gave to WMP adequately reflected their experiences on the day of the disaster with a “yes”.
However, 490 answered this question “no”. Following further contact with these witnesses, the IOPC recorded complaints in relation to various issues.
36 witnesses stated the officers did not accurately or adequately record their responses.
18 witnesses complained about the overall attitude of officers.
15 witnesses complained that officers focused excessively on supporters’ alcohol consumption.
10 witnesses stated that when they tried to make complaints about the actions of SYP officers, these complaints were not recorded or subsequently investigated.
7 complaints referred to WMP officers interviewing witnesses under the age of 18 without an adult being present.
2 complaints related to the fact that, after the complainant had called the IIC, WMP did not follow up their initial information in any way.
Several of the complaints related to more than one issue and some were subsequently discontinued at supporters’ request.
As part of its investigation, the IOPC researched each pair of officers who took statements and questionnaires from witnesses to explore whether any were subject to higher numbers of complaints. There were no officers that were subject to particularly high numbers of complaints, which indicates there was no specific pattern of behaviour.
WMP first used questionnaires in relation to the disaster in the incident information centre (IIC) that it opened on 18 April 1989. This was, in effect, an incident ‘hotline’, based at a WMP police station. On 22 April, ACC Jones recorded in his policy book that witnesses who called the IIC would be asked to answer a questionnaire. This consisted of just nine questions and was effectively a preliminary assessment of whether the caller should be interviewed in person.
By 25 April, WMP had decided that questionnaires would be used more widely in gathering evidence from supporters. A questionnaire was developed consisting of 54 questions, covering topics such as:
whether supporters had been delayed on their journeys to the stadium
the time at which supporters arrived in Sheffield and then at the ground
police direction outside the ground
recollections of entry to the ground and the opening of the gates
police and steward control inside the ground
the crush barrier breaking
One of the main recurring allegations related to WMP’s evidence collection in Merseyside was that officers focused excessively on supporters’ alcohol consumption. The questionnaires used for both Liverpool and Nottingham Forest supporters had three questions that mentioned alcohol or drunkenness.
Did you witness prior to arrival at the ground any other supporters consuming alcohol?
Did you witness any disorder, fighting or drunkenness between your arrival point and the ground?
Did you witness any consumption of alcohol in the ground? If so, briefly explain.
Notably, there was no question directly asking supporters if they had drunk alcohol. Question 9—“Did you stop anywhere en route to the game, if so where and for what purpose?”—could be viewed as an attempt to secure that information.
This stood in stark contrast to the fact that almost 1 in 6 respondents to the IOPC witness appeal reported that WMP officers focused disproportionately on supporters’ alcohol consumption.
Separate questionnaires were developed for use with other categories of witness, including SWFC stewards and turnstile operators, and local residents in the area around the stadium. Several hundred questionnaires were completed with these groups of witnesses. The IOPC did not receive any complaints about WMP’s approach with regard to these.
As well as using questionnaires, WMP’s intention from the start was to take formal statements under Criminal Justice Act rules (CJA statements) from witnesses in certain circumstances. It only submitted witness statements to the Taylor Inquiry; the questionnaires were effectively a screening tool to help determine whether a statement should be taken from the witness. The IOPC has not found any specific document that instructed officers when they should do this. Some WMP officers have indicated that the decision was left to them, when they were interviewing witnesses; others referred to being given specific instructions to take a statement, either as part of the first visit to a witness, or as a follow-up after the questionnaire had been examined. In practice, it seems likely all three applied.
However, it does appear that WMP officers did not always inform witnesses that they were using a questionnaire rather than taking a statement. This was raised by many respondents to the IOPC’s witness appeal who had not been able to find their statement on the HIP’s online document repository.
The IOPC was able to explain this and reassure many of the witnesses. For data protection reasons, the HIP had removed the names of most witnesses before publishing the documents. IOPC investigators had access to the original versions of all statements and questionnaires, which included the names of the witnesses. They could therefore find any statement or questionnaire registered by WMP in the respondent’s name or identify where it had been published by the HIP and send it through. In many cases, this was sufficient, and the witnesses had no further concerns.
A team of WMP officers first arrived in Sheffield on 18 April 1989. Early steps included securing the stadium as a crime scene, setting up an MIR and meeting with some of the senior SYP officers who had been involved in collecting evidence up to that point. During that morning, CC Dear took part in a press conference with Lord Justice Taylor, which explained the remit of the Inquiry and WMP’s role in it.
At 2pm, ACC Jones recorded a policy decision that “the limits of the South Yorkshire Police enquiry should be to the preservation of evidence and no further.” He then expanded on that in a subsequent policy decision the same afternoon, which again focused on “preserving evidence”; he added that no interviews would be undertaken at that stage.
On 19 April, WMP began to take over the investigation. The transition took a few days to complete. In a later letter to the South Yorkshire Joint Secretariat (the body that provided shared services, such as legal services, to various public authorities in South Yorkshire), Ch Supt Denton recalled that on 20 April, Detective Superintendent Roy Taylor of WMP (D Supt Taylor) instructed that all enquiries by SYP officers must be suspended. On 22 April, the SYP HOLMES account was closed and all data backed up to tape. The tapes were handed over to WMP and retained with other material. Then, on 24 April, all the documents and exhibits SYP had collated were also passed to WMP.
The IOPC has not found evidence to indicate there was anything inappropriate or unprofessional in this transfer of responsibility and evidence.
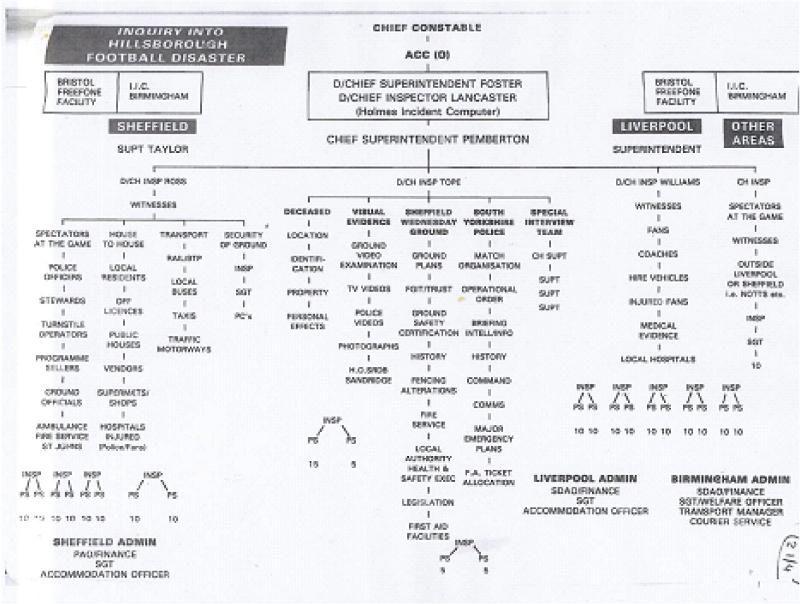
Alongside the activity in Sheffield, back in Birmingham, WMP had begun to plan its approach to gathering information. A team of senior officers worked together to identify lines of enquiry and consider staffing requirements. They produced a chart summarising these, which was included in ACC Jones’s policy book and is shown as figure 14A.
None of the topics included stands out as unusual or inappropriate in the context of investigating the disaster.
To gather information consistently from large numbers of witnesses, WMP chose to use questionnaires. These were a standard investigative tool, but the questionnaires in this case were mentioned in numerous complaints to the IOPC about WMP’s work.
WMP first became involved in investigating the Hillsborough disaster on 16 April 1989, when WMP’s Chief Constable Geoffrey Dear (CC Dear) was asked by CC Wright to examine SYP officers’ planning for the match and operational decisions on the day.
On 17 April 1989, it was announced that WMP had been further appointed by the Home Secretary to support Lord Justice Taylor in his inquiry into the disaster. Almost immediately after that, WMP was also appointed to support Dr Popper in the inquests. At this stage, no criminal or disciplinary investigation had been started.
Though the choice of WMP for these tasks was swift, the IOPC has not found any definitive explanation of why WMP was nominated, nor found any evidence to suggest that the decision was biased or inappropriate.
WMP was a large force with considerable experience of policing major football matches. It had five football grounds in its area, one of which was Villa Park, the venue for the other FA Cup Semi-Final in 1989. Further, CC Dear was a highly experienced officer who had been involved in several high-profile investigations and inquiries and was well regarded by the Home Secretary, Mr Hurd.
CC Dear and CC Wright did know each other through police circles, but when interviewed by the IOPC, CC Dear stated there was no particular friendship or professional relationship between them. They had not served in the same force at any point, and no evidence has been found to indicate they were close.
In addition to the witness appeal, the IOPC also had a second major source of new evidence: the policy books of ACC Jones, who led WMP’s work around the disaster.
This was a series of 14 physical notebooks into which were attached detailed, chronological records of ACC Jones’s correspondence, telephone calls and meeting notes throughout the investigations. They also included some policy decisions, often flagged as such, among more detailed entries. Each entry was numbered, and they appeared to form a continuous record of how WMP conducted its work, the decisions made by senior officers and its dealings with other parties, including SYP, the Taylor Inquiry team and Dr Popper.
The policy books therefore were of considerable importance to the IOPC’s investigation into WMP’s work.
The books were provided to the IOPC by ACC Jones in 2013. He had retained them in his personal possession when he left WMP and had not previously made them available to any other party, investigation or review of evidence relating to the Hillsborough disaster.
Though he had not been specifically contacted by the Stuart-Smith Scrutiny, there is evidence that he was aware of its work and aims. In 2011, the HIP contacted ACC Jones and asked if he had any relevant material for its work. He did not provide the policy books and advised the HIP that “all of the product of my involvement in the investigation” had been retained by WMP.
He later told the IOPC that when the HIP contacted him, he had forgotten he had them. He further said that the policy books were “my copies of material forwarded to the official Holmes Policy File”, adding: “the contents you have probably found are already known to you from the official file.” In short, he suggested that the policy books were only duplicates and that the material in them would all have been available elsewhere.
While the HIP did have access to copies of many of the documents in the policy books, it did not have all of them. Further, when the IOPC restored and examined the HOLMES databases used by WMP for its work around the Hillsborough disaster, it became apparent that ACC Jones had requested that some of the electronic policy files related to WMP’s investigation should be deleted from the system. Before doing so, he requested that printed copies were made.
An officer retaining potentially sensitive material relating to police work in their personal possession, and deleting material from the HOLMES system, are both unusual steps.
Further, given the allegations of a failure in the direction and control of WMP’s investigations noted in WMP’s referral to the IOPC, the deletion appeared particularly significant. It was therefore one of the issues raised in the Notice of alleged breach of the Standards of Professional Behaviour the IOPC sent to ACC Jones in January 2015.
ACC Jones responded to the allegation in a prepared statement to the IOPC. He stated that the deletion of the policy files had been agreed as they contained potentially sensitive and confidential material. However, he provided no further details, such as who this had been agreed with. He also said he did not have the printed copies of the policy entries.
Given the potential value of the policy files, and the strong indication that they were not the same as the policy books, the IOPC carried out or requested a number of further searches in an attempt to find them, in either digital or hard copy format. This included searches of police premises and obtaining a warrant to search ACC Jones’s home. The files were not recovered.
Though ACC Jones’s decision to delete the files was documented and included an instruction to retain hard copies, it was nonetheless highly unusual and leaves a gap in the IOPC investigation. It remains unclear what happened to the hard copies of the policy files.
The IOPC recorded a conduct matter around ACC Jones’s actions and completed an investigation into it. Having reviewed the investigation report, the IOPC was of the view that, if he had still been serving, ACC Jones would have had a case to answer for gross misconduct for discreditable conduct in relation to the deletion of the files, falsehood or prevarication regarding the retention of the policy books and neglect of duty, because he did not advise the Stuart-Smith Scrutiny of the books’ existence in 1997.
Though the IOPC had access to thousands of archive documents relating to the investigations, there was comparatively little evidence within these documents about how WMP conducted its investigations. To address this, in September 2013, the IOPC launched a witness appeal, inviting people who had any contact with WMP during its initial investigation to contact the IOPC and share their accounts and experiences. This became the largest witness appeal the IOPC had ever conducted. In total, 1,713 individuals responded, of whom 1,325 said they had some dealings with WMP. Many of those who responded had never previously given an account to any inquiry or investigation.
Every respondent who had contact with WMP was asked if they believed the account they gave to WMP adequately reflected their experiences on the day of the disaster. While over 800 respondents said it did, 490 answered this question “no”. These individuals were then asked why: a range of reasons were given, with some giving more than one reason.
Those who said “no” were contacted again by IOPC investigators who asked for more information about the reasons for their dissatisfaction. Before contacting them, the IOPC investigators examined archived material and the WMP HOLMES databases to retrieve any statement or questionnaire registered by WMP in the respondent’s name. Investigators then sent the respondent a copy of these documents or, where the documents had already been published on the HIP website, directed them to the relevant pages.
In many cases, the dissatisfaction expressed specifically related to the fact that the respondent recalled being interviewed by WMP but had not been able to find any documentation related to them. One reason for this was that, in many cases, the HIP redacted the names of witnesses before publishing the documents. Once they had confirmed that there were documents that related to them, many of these witnesses informed the IOPC that they had no further issues.
However, over a quarter of those who had engaged with WMP expressed concerns about the behaviour and manner of the officers who interviewed them. Other common concerns raised by respondents were that WMP officers:
interviewed witnesses, but did not take a formal statement from them
did not record witnesses’ evidence accurately
appeared uninterested in what the witness had to say
focused excessively on alcohol consumption
interviewed witnesses under the age of 18 without an adult being present
Arising from these concerns, the IOPC received 66 formal complaints relating to these issues. This meant that WMP’s approach to collecting evidence from supporters for the Taylor Inquiry was the most common source of complaints related to the Hillsborough disaster.